

| Equine Dentistry 6 August, 2012 – Dr Helen Tiffin |

Equine Dentistry was the very origin of the veterinary profession more than a century ago, now recently in the last 20 years there has been a major resurgence of interest in dentistry with a large amount of research being done.
Dental disease in horses is a major cause of problems and there is some controversy over whether vets or dentists are best suited to do this work.
Horse’s teeth are called hypsodont (high crowned) and they continuously erupt throughout the life of the horse. After losing the deciduous teeth the permanent teeth erupt and take their place.
There is a finite length to the permanent teeth and once the full length of the tooth has been lost it is gone.
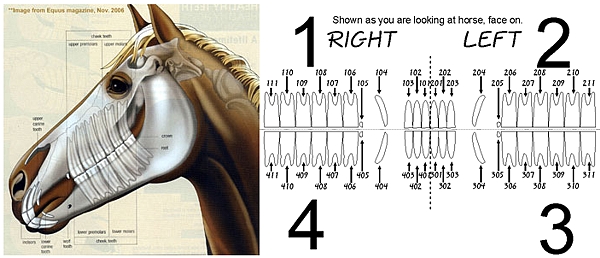
There are 44 teeth in the equine mouth, labelled in a modified Triadan system as illustrated below.
Clinical signs of dental disease are only seen when the condition is advanced, routine dental care should prevent this stage being reached. Clinical signs seen are accumulation of food in the cheeks, halitosis(bad breath), chewing slowly with slurping noises, quidding(dropping partially chewed food), weight loss, facial swelling, unilateral purulent nasal discharge and at worst draining tracts.
When examining the oral cavity a Hausmann’s Gag (full mouth speculum) is essential allowing a thorough examination. Oral endoscopy is becoming beneficial in diagnosing subtle lesions such as small fissure fractures, pulpar abnormalities and diastema. X-rays, when indicated, are an important diagnostic tool to evaluate the deeper structures such as the apex of the tooth and sinuses.

When preventing, treating or correcting abnormal dental conditions ‘less is more’! Remember there is a finite length of tooth in the horse and it is a major limiting factor in the longevity of the life of the horse. Excessive lowering of the tooth may also cause exposure of the sensitive pulp cavity causing discomfort and allowing infection of the pulp cavity. Reductions of over grown, or rather under worn, teeth needs to be done carefully with only 2-3mm reduced at a time to avoid exposure of the pulp horns.
The most common condition treated is sharp enamel points on the molars. These develop on the buccal(cheek) side of the maxillary arcades (which are wider) and lingual(tongue side) of the mandibular arcade (which is narrower). They often cause ulcers and damage to the corresponding cheek mucosa, especially if associated with tight nosebands.
Enamel is the hardest substance in the body and with its irregular occlusal surface creates its own self sharpening system with the softer cementum and dentine creating ridges allowing efficient mastication of hard fibrous material. If this wearing surface is smoothed off mastication is inefficient or even painful.
Hooks/ramps are most often present on the rostral (front) aspect of the maxillary 06s and mandibular 11s. These need to be carefully lowered but are important to correct. They can interfere with bitting, cause stress on the temporomandibular joint (TMJ) and in performance horses makes the head position of working in a frame uncomfortable and even painful. They should only be reduced to the occlusal surface of the tooth allowing a greater lateral excursion.
The creation of ‘bit seats’ or ‘rostral profiling’ should be done judiciously with only a rounding off of the rostral 06s. Excessive rasping once again risks exposing pulp horn.

Diastemata are a common dental disorder where food material impacts between teeth and are regarded a most painful oral disease in horses resulting in gingivitis and damage/infection of the periodontium.
They may develop secondary to an adjacent displaced tooth, missing tooth or a senile development as the tooth tapers near the apex.
Small Wolf Teeth rarely cause problems but larger ones or more cranially situated ones can interfere with the bit. They are the first premolars (05s) with a small shallow root and can be extracted under local anaesthesia; care must be taken not to lacerate the large palatine artery.
The Canines seldom require floating which may cause pulp exposure. They are difficult to extract due to their large reserve crown (root) and if it needs to be done should be done under GA.
The Incisors rarely cause dental disease but if it is present is often noticed easily as they are easily visible. They rarely need floating, and only once the cheek teeth problems are corrected should they be adjusted.

Brachygnathism (parrot mouth) and less often Prognathism (under shot jaw) may result in over growth of the incisors if extreme. More importantly they are associated with uneven alignment of the cheek teeth as the whole jaw is displaced with the resultant development of large hooks. The presence of ‘slant’, ‘frown’ or ‘smile’ mouth are indicative of disorders in the cheek teeth. The abnormal mastication caused by the cheek teeth lesion results in abnormal wear of the incisors making them secondary to the cheek teeth disorder.
Routine dental care (every 6 to 12 months) will recognise these conditions early in their development and limit their degree of severity and impact on the horse keeping him happy, healthy and performing well.

Bosch Hoek Equine Hospital is a state of the art Equine hospital situated in the beautiful Kwa-Zulu Natal Midlands of South Africa. Our primary goal is to offer clients and their horses world class care and expertise for both surgical and medical conditions with a rehabilitation centre to match.
If you require our services or would like to discuss anything please call one of us on the numbers below:
Dr Helen Tiffin 082 966 9324
Dr Jenny Lawrence 082 836 9897
Dr Anna Bowker 082 849 3456 (away until August)
Dr John Hodsdon 072 165 7122
 Dr Helen Tiffin Dr Helen TiffinEquine Veterinarian Born with a passion for horses, Helen worked in the equine industry for several years before studying to become an Equine Veterinarian. After qualifying in 2004, Helen began work with the Equine Research Centre in Pretoria. In 2005 she joined Dave Mullin’s practice in the KZN Midlands where she became a valuable asset to the equine community. Helen has continued riding throughout and competes regularly at local events when time allows. |